

Dento-Aveolar Trauma
Dento-alveolar trauma is relatively frequent and is usually associated with soft tissue trauma. It is an urgent condition. In fact, the prognosis of traumatized teeth depends on the delay between the accident and treatment time. The health professional, after having established the circumstances of the event, will proceed with a clinical examination and take X-rays.
In some cases, the traumatic injury is limited to the teeth, in others the teeth and supporting bone are injured. In most cases, the initial treatment involves the repositioning of the teeth in the dento-alveolar process followed by immobilization with arch bars or acrylic splints. Depending on the amount of displacement, the immobilization period could be from 2 to 4 weeks. Regular follow-up visits to the dentist during the first years after the trauma are important to assess and treat any problem with the healing of the injured teeth including pulp necrosis or mobility.
Cranio-maxillofacial trauma
The most common causes of maxillofacial trauma are high velocity accidents, falls, sports’ injuries and altercations. They include simple non-displaced fractures needing only observation to multiple and complex fractures of the facial skeleton resulting in severe sequelas if left untreated.
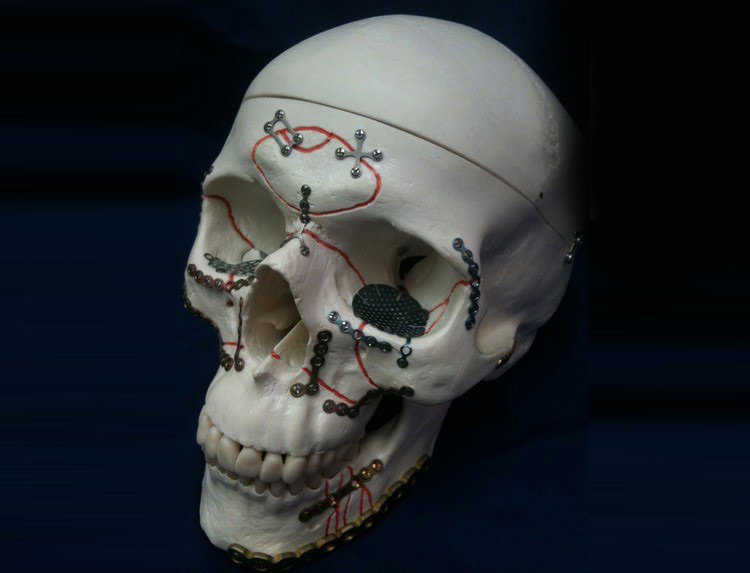
Depending of the situation, open reduction and internal fixation of the fractures with plates and scews might be indicated. Facial fractures are divided in three main categories:
fractures of the lower third (the jaws: maxilla/ mandible), middle third (nose and cheek bones) and upper third (orbital and frontal bones).
Different intra-oral and extra-oral approaches are used to access the fractured bones and allow for fixation. The main objective of repairing facial fractures is to re-establish function and esthetics.