
Obstructive sleep apnea syndrome (OSA) is a sleep disorder characterized by periods of respiratory arrest (Apnea) or decreased air-flow (hypopnea) leading to oxygen desaturation in the blood.
OSA affects approximately 4% of men and 2% of women aged between 30 and 60 years old. This percentage increases to 28 to 67% in older men compared to 20 to 54% in older women. An important discrepancy exists between the estimated prevalence of OSA and the patients accurately diagnosed and treated, where an estimated 80% of patients with moderate to severe OSA are not diagnosed.
Apneas occurring during sleep can take two forms: Obstructive apneas, are caused by an anatomical obstruction of the upper airway, central apneas are related to a decreased respiratory drive in the brain-stem during sleep and a mixed apnea can be a combination of both. Apnea itself is defined as absence of breathing for 10 seconds or more despite respiratory effort. Hypopnea is resultant to a reduction of 30 to 50 % of respiratory flow for at least 10 seconds with a resultant 3-4% oxygen desaturation. The severity of OSA is classified according to the Apnea Hypopnea index (AHI). AHI is the average number of apneas and hypopneas per hour of sleep. AHI of greater than 5 and less than 15 is mild OSA, while 16-30 is moderate and greater than 30 is severe.
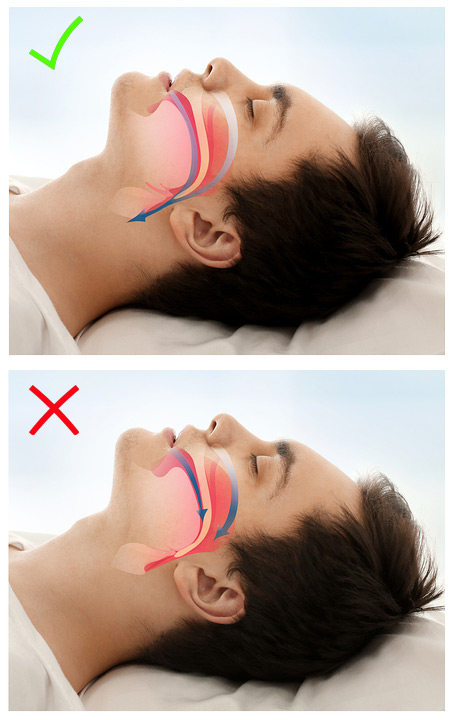
The obstruction of the upper airways can happen at multiple levels; the nasal region, the retro-palatine region and the oropharynx. Obstruction at the level of the nasal region, can be caused by a deviated septum, hypertrophic lower turbinates or narrow nasal floor. The retro-palatine region is the most common site of obstruction in teenagers and kids due to hypertrophic adenoids and/or tonsils. Also, a hypoplatic maxilla can decrease the volume of the nasopharynx, especially in patients with cleft lip and palate who are at higher risk of developing OSA. The oropharynx or posterior airways space is largely affected by the anterio-posterior position of the mandible and tongue. A retrognathic mandible causes the tongue to be positioned posteriorly which can cause obstruction at the level of the oropharynx during sleep. Other risk factors for OSA include a macroglossia (Hypertrophic tongue), obesity (BMI > 34), advanced age, family history of OSA, excessive alcohol consumption and cigarette smoking. Men are at higher risk for OSA due to differences in the anatomical and functional characteristics of their upper airways' structures and the respiratory response to micoarousals.
