

Cleft lip and palate
Cleft lip and palate (CLP) represents the most common congenital malformation of the face. Its incidence is estimated at 1 case per 500 to 1,000 births. Asiatic and aboriginal populations have a higher incidence compared to caucasians and African Americans.
This malformation affects both the lip and palate in 46% of cases. Thirty three percent involve the palate only and 21% are isolated cleft lips. CLP is more often unilateral (left side) and affects males more than females in a 2:1 ratio.
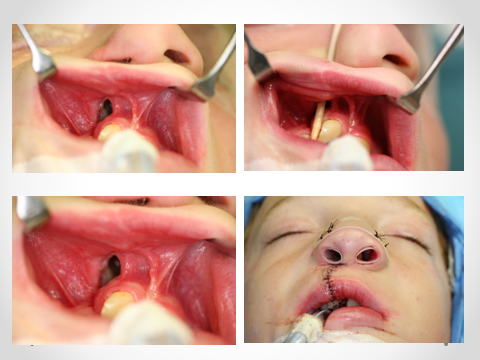
The alveolar bone graft at the cleft site will provide:
- Continuity of the alveolar bone of the upper jaw
- Bone support for the eruption of teeth adjacent to the cleft
- Bone support for possible future dental implants
- Closure of the oro-nasal fistula
The expertise of the oral and maxillofacial surgeon is called upon once again when patient’s growth has ceased and jaw corrective surgery is needed. Patients with CLP usually have a retrusive upper jaw; jaw corrective surgery is recommended is these cases. Moreover, the oral and maxillofacial surgeon will repair any residual oro-antral or oro-nasal fistula, graft deficient alveolar ridges, or perform cheilo-rhinoplasty.
Figure 1 Oronasal fistula cure, image courtesy of Dr. Valcourt*
Craniofacial syndromes
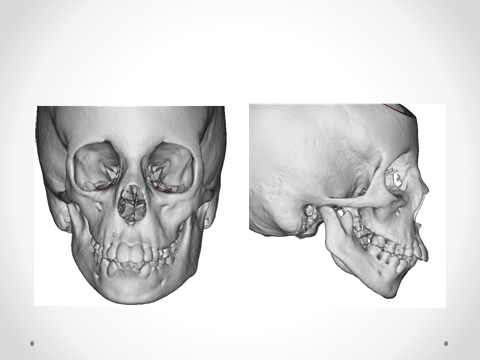
Hemifacial macrosomia is a deformity belonging to the spectrum of Goldenhar Syndrome (oculo-auriculo-vertebral dysplasia). It involves a unilateral hypoplasia of the face and affects mainly the middle and lower thirds.
This syndrome is associated with varying degrees of hypoplasia: the hypoplasia could lead to agenesis (complete absence) of the mandibular condyle as well as other parts of the lower jaw. The Goldenhar syndrome could also be associated with cleft lip and palate, hypoplasia or absence of different structures of the external and middle ear. The muscles and salivary glands on the same side also present varying degrees of hypoplasia. Goldenhar syndrome is confirmed when cardiac, cervical, and ocular anomalies are diagnosed.
Figure 2 Hemifacial microscopy, indicating the hypo-development of the right mandible. image courtesy of Dr. Valcourt*