
Description of the temporomandibular joint
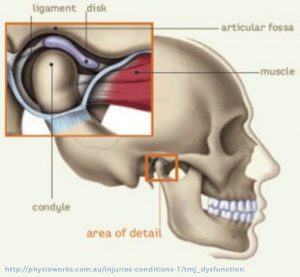
The temporomandibular joint (TMJ) is the articulation of the lower jaw. Its two bony structures are: the mandibular condyle and the glenoid fossa in the cranial base. Interposed between the two is a cartilaginous disc called the articular disc. All these structures are surrounded by a dense fibrous capsule.
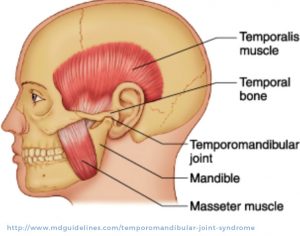
Masticatory muscles
The masticatory muscles are responsible for mouth closure. The two main ones are the masseter and temporalis muscles
Description of TMJ disorders and Myofascial pain syndrome
These disorders affect one of more of the TMJ structures and the masticatory muscles.
This is a musculo-skeletal pain characterized by local tenderness and referred, deep and constant pain. The pain is sometimes elicited by palpation of trigger points in the affected muscles. The referred pain is a perceived pain in a different region than the site of origin of the dysfunction.
This involves the anterior displacement of the articular disc caused by the stretching of the posterior articular ligament. Over time, the displacement can interfere with mouth opening. The usual signs and symptoms are: pain, articular click, and difficulty with full mouth opening.
Although much of the population experiences a cracking sound when opening their mouth, few require treatment. If a cracking joint is present without limitation to mouth opening and without pain, the disc displacement is usually diagnosed as an anterior disc displacement with reduction; the disc will recover its normal position on the condyle when the mouth is opened.
However, in some cases patients have pain and difficulty opening their mouth. This most probably represents an anterior disc displacement without reduction which is due to a disc that is severely displaced and does not recover its normal position upon opening. In these situations, the disc will interfere and prevent the condyle from moving, therefore limiting the mouth opening. It is important to note that anterior disc displacement with reduction will not necessarily progress to anterior disc displacement without reduction.
These are degenerative changes of the articular surface. They usually manifest as TMJ pain exacerbated by chewing, yawning, and speech. Crepitus of the TMJ is a common symptom; it is the result of a rubbing between the articular surfaces that have lost their smooth aspect. In severe cases, pain is present and there is limited mouth opening. Extremely severe cases are associated with occlusal changes and facial asymmetry. Degenerative TMJ disorders can be idiopathic,
a result of chronic disc displacement, or the manifestation of autoimmune diseases like rheumatoid arthritis.
This is due to an excessive condylar movement that results in the displacement of the condyle out of the articular fossa (glenoid fossa). If the condyle can return to the glenoid fossa spontaneously the condition is called a TMJ subluxation. It is secondary to hyperelasticity of the articular ligament. In cases where the condyle is locked out of the fossa, the condition is called an open lock. The patient is unable to close his mouth and needs to be seen by a health professional for a manual manipulation to help close the mouth.
This is due to the fusion of the two bony structures of the joint: the mandibular condyle and the glenoid fossa. This rare phenomenon is secondary to the replacement of the articular surfaces by fibrous or osseous tissue. Generally, this condition is non-painful but causes a severe limitation in mouth opening. It could be the result of trauma, infection, or rheumatoid process.
If the condition affects growing patients, it will present – on top of speech, nutrition, and dental hygiene issues – abnormal growth of the jaw that can lead to facial asymmetry.
Treatment options
These disorders affect one of more of the TMJ structures and the masticatory muscles.
This consists of anti-inflammatory drugs (NSAIDs) and muscle relaxants. Physical therapy is also an essential component of this approach. In addition, patients are also instructed to stop parafunctional habits like clenching and nail biting. Moreover, changes in the diet to soft, non-chew food and avoiding chewing gum is recommended. An occlusal splint could be indicated. Regular follow-ups are important. Obviously, a follow-up with your surgeon is necessary.
Injections of type-A botulinum toxins are used for patients with myofascial pain syndrome. In fact, when injected in tension zones in the masseter and temporalis muscles, masticatory forces are decreased, the muscle becomes less tense leading to interruption of the inflammatory process. The effect is temporary and usually lasts for a maximum of 3 months.
This consists of injection of corticosteroids within the joint space. Corticosteroids are potent anti-inflammatory drugs. These injections are done in the clinic with or without intravenous sedation.
Arthroscopy: This procedure is done under general anesthesia. The surgeon inserts a camera in the joint space to diagnose and evaluate the articular damage. At the same time, a joint lavage could be done to wash inflammatory mediators that trigger and maintains the inflammation inside the joint. Also, the hydraulic pressure of the articular lavage will help break fibrous adhesions that restrict articular disc movement.
Arthrocentesis: This is usually done in the outpatient clinic under local anesthesia or intravenous sedation. It is similar to the articular lavage done during arthroscopy but does not include the introduction of scopes to visualize the inside of the joint.
Open TMJ surgeries: All these surgeries consist of surgically opening the joint through a pre-auricular approach to directly visualize the components of the TMJ. Different techniques can be used to repair the affected joint depending on the diagnosis. For problems involving the disc, repositioning (meniscopexy) or complete ablation (meniscectomy) are done. The articular eminence could be modified to improve function: eminectomy or Bute d’Autrey. Arthroplasty is used to eliminate irregularities of the joint surfaces. Finally, in severe degenerative cases, a total joint replacement with alloplastic joints or costochondral grafts could be offered.